Traditional western medicine has such an allure. It seems so logical and certain, backed by peer-reviewed studies, meticulously planned experiments, and intimidating scientific jargon spoken by the highly educated—and those authoritative white coats! It’s true that when we have surgery, we sign a form that lists possible bad outcomes, attesting that we are aware of them, but we know that, mostly, none of them happen. The heart starts pumping effectively again; the elbow allows tennis to be played; the tonsils no longer disrupt sleep. Take a problem to a doctor, the doctor diagnoses it, the doctor fixes it, and life goes on.
But then there is a condition like mine. I still recall the just-a-tad-too-long sigh that the nurse practitioner gave at the ENT office when I first told her I couldn’t taste or smell. The kind of sigh—along with that wondering quick look around the room—that gives the speaker an extra couple of seconds to figure out how to tell someone something they don’t want to hear. “That’s tricky,” she said.
Tricky. It’s fun when magicians trick us. Not so fun when our bodies trick us.
According to doctors I saw, I was past the point when my taste and smell might return on its own—perhaps by the olfactory nerve restoring itself—but, regardless, I visited a clinic in another part of the country that specializes in taste and smell problems. I went out of desperation, hoping they would find some something that the others had missed and say, “Aha! Take this pill, and you will savor Ben & Jerry’s New York Super Fudge Chunk again.” I knew that wouldn’t happen, but, still, I went.

The first day, a lab clinician sat next to little jars of liquids and solids. The bottles clinked as he pulled them from their slots and when he returned them. I sniffed in alternating nostrils, and I swirled liquids in my mouth, trying to identify smells and tastes. In one test, he had a list of aromas (coffee, chocolate, peanut butter, etc.), and I was to take a sniff of an opened unmarked bottle and choose which one it was. (Eventually, he remarked, “You really like to guess peanut butter, don’t you?”) In another test I was to say if a clear liquid was sweet or sour or salty. I was pretty good at that one, and I was quite keen at identifying sour. These tests went on for two and a half hours.
Mostly, I just guessed, like a 10th grader who forgot to study for a multiple-choice quiz. The olfactory and taste feedback were just so minimal. Although I had been told already that by this time the loss was permanent, the repeated failure on these tests made the reality of the loss sink in even deeper. Each time I sniffed or swirled in vain, the message became clearer.
According to the report on these tests, my left nostril correctly identified baby powder, cinnamon, mothballs, peanut butter, and Ivory soap. The right nostril only got right baby powder, chocolate, and coffee. I believe many of those were lucky guesses. During most of those tests I felt like I had felt in college biology class: bewilderingly ignorant of what was going on.


The next day was a free day. I toured some local historic sites and visited an old friend from my seminary days in the 1980s.
The day after that, I saw two doctors, one who did a complete physical exam and the other, a taste and smell specialist. The first doctor and I chatted about where we liked to snow ski while he conducted his exam. The specialist went over the results of the Wednesday tests and conducted his own exam, including taking a deep look in my nostrils, using what looked like a chopstick to pry each nostril open wider.
These clinicians never asked me my religious affiliation, but their medical record of me inexplicably, even though I am a practicing Baptist and an ordained minister, says in that category: “NO.” Unless they were sneakily very astute, we never discussed anything outside the taste and smell problem, but in my medical record, under “Constitutional,” it says: “No acute distress. Well nourished. Well developed.” Under “Psychiatric,” it says, among other things: “Not in denial. Not euphoric. Not fearful. No flight of ideas. No grandiosity. Not hopeless. No mood swings. Not paranoid. Normal insight. Normal judgment.” And: “Behavior is appropriate for age.” (I’m not sure about that one; I still like to watch “Green Acres” and “Gilligan’s Island.”) At least I make a good—albeit agnostic—impression.

I have “rightward septal deviation”—a crooked nose, not bad enough to require surgical repair, however. I can breathe OK. I have “mild hypertrophy of turbinates bilaterally” (both nostrils). Turbinates are rollicking little items inside our noses, which humidify, heat, and filter the air we inhale. Our lungs, apparently, are particular. They like their air the way I (used to) like cinnamon rolls: clean, warmed just right, and moist.
Detroit’s Henry Ford Health System web site describes turbinates this way:
“Turbinates are structures located inside the nose, along the sides of the nasal cavities. They are made of bone and are covered by soft tissue known as ‘mucosa.’ Their function is to regulate airflow, and to warm and humidify the air you breathe in….Turbinates achieve this in part by swelling up periodically with increased blood flow, and this process characteristically alternates between sides every few hours (called the ‘nasal cycle’). This results in airflow being temporarily restricted on one side before alternating to the other side. This is one reason patients may feel their nasal obstruction ‘switches sides.’…There are three pairs of turbinates, inferior turbinates being the largest and located lowest in the nose. If the inferior turbinates are too large…they can cause nasal obstruction in one or both sides of the nose.”

So, to sum up what is likely more information than you want about the inside of my nostrils, my turbinates are a little larger than normal but not so much that I can’t breathe well.
(Here’s a fun medical fact: If your turbinates are enlarged enough to require partial removal and the doc accidentally removes too much, you may have “empty nose syndrome,” wherein even though the nostrils are wide open, without the proper mechanism to sense air flow, you will think your airway is obstructed.)
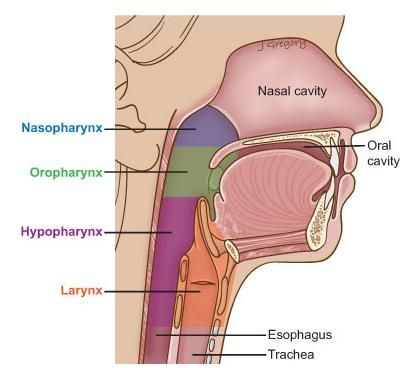
One last roll-out-the-jargon diagnosis: I have “pseudosulcus bilaterally upon examination of hypopharynx and larynx.” Whew.
As a college professor once said, let’s unpack that (or, in this case, have two websites unpack it for us). According to the American Cancer Society, “The hypopharynx is the part of the throat (pharynx) that lies beside and behind your larynx. The hypopharynx is the entrance into the esophagus (the tube that connects the throat to the stomach). When you swallow foods and liquids, they pass through your mouth and throat, through the hypopharynx and esophagus, and then into your stomach. The hypopharynx is made so that it helps make sure that food goes around the larynx and into the esophagus.”
And per Wiktionary.org: pseudosulcus (plural is pseudosulci) means: “A groove that has the appearance of a sulcus,” which is no help because a sulcus is itself a “groove or furrow,” according to dictionary.com—and they can be in lots of places in our bodies. After many internet searches I gave up on finding a layperson’s definition of pseudosulcus bilaterally upon examination of hypopharynx and larynx. All I know is that it is not relevant to my loss of taste and smell, and it is not a concern of the doctors. I’m just a groovy guy and, in one spot, pseudo-groovy.
They detected signs of acid reflux (the pseudosulcus was one sign), and they recommended diet changes. (I made that change, which did reduce the acid reflux.) According to the Schirmer test, my tears are normal, and according to the Saxon test, my saliva is normal. I can cry and spit just fine. Hallelujah.
I learned that I can smell better in one nostril than the other—something I didn’t know was possible. Apparently, each nostril stays separate from the other longer than I thought, and can function differently. My left nostril has “mild hyposmia,” and the right nostril, the more pitiful smeller of the two, has “severe hyposmia,” hyposmia being a reduced ability to smell and detect odors—less traumatic than anosmia, in which no odors whatsoever can be detected.
They diagnosed “whole mouth hypogeusia without focality.” “Without focality” means there is no spot to point at and say, “There’s your problem, right there.” Hypogeusia is a diminished loss of taste—which, if one is inclined to look for silver linings, is not as bad as ageusia, the complete loss of taste.
While not having anosmia or ageusia—that unsatisfying and disappointing empty abyss of a gastronomic experience—is good, I suppose, it leaves me in a frustrating middle ground. I can sort of taste a few things if the taste is strong enough. But I can’t taste most things, and, among those that I do, I don’t really taste them in the “oh that’s yummy” way that is the reason we eat delicious food. We don’t robotically say, “I will ingest this fuel that is necessary for functioning. My body will keep what it needs and output the rest.” We salivate; we crave good food.
About those tastes that I can faintly detect, usually, the most I can say is: I know they’re there. Which is not satisfying. Sometimes I can tell what something is by texture, as with an apricot with its specific mushy-chewiness. Blindfolded, I can tell whether coffee I sip has cream added; blindfolded, I can tell if a hamburger has pickles. I can tell they’re there, but that’s about it. It’s like hearing the faint through-the-walls sounds of your favorite music band which your friends are ecstatically enjoying inside the arena while you’re standing outside on the sidewalk, ticketless.
Chocolate is pretty distinct, and I can tell it is sweet. There’s still something in my brain that says, “That’s sweet,” and, according to nutritionist Diana Sugiuchi, “Our brains are biologically programmed to seek out sweets. Eating sweets activates the same receptors in your brain that morphine and heroin do, but it’s easier to get your hands on chocolate.”

So my brain, perhaps desperately addicted, demands sweets and is immediately disappointed by their consumption. Every now and then I’ll eat something sweet (crunchy + gooey can compel me over there) then promptly think, “That was a letdown.”
The clinic, as expected, didn’t provide an answer to why this happened to me. They suspect a “silent viral infection” but don’t rule out a fall I had while skiing.
They suggested I try aroma therapy: sniff 4 or 5 strongly aromatic compounds such as coffee grounds, peppermint, vanilla extract, and peanut butter, 5-10 minutes twice a day. (I tried that—no change.) They said get a gas leak detector and be cautious about spoiled food.
I submitted to the medically specialized tests and observations and opinions that we, usually, count on to save us, but this condition eluded their ability to apprehend and resolve. They drew conclusions about me regarding religion, personality, and psychology without asking me anything personal or engaging me about how I am coping. I didn’t visit the clinic for those reasons, but I found it odd that they included these matters in their conclusions without any related inquiry.
It was time to try something else.
I haven’t much tried alternative medicine (there is a debate about what to call it), not because of disbelief or skepticism but more out of upbringing and habit. I have had friends who scoffed at it and friends who praised it. I haven’t joined the fray. But missing out on the sauteed snow pea leaves, chicken in clay pot, and salt-and-pepper shrimp at our favorite Chinese restaurant was enough to jolt me out of my assumptions and habits. I asked around about acupuncture, and a friend recommended someone she had seen. She said, “He helped me. Plus, I liked what he had to say.” That is next.

